Cancer clinical trials are supposed to yield evidence about the benefits and harms of new treatments. “By accident or design, the current system seems to achieve the exact opposite,” in the words of Richard Lehman and Cary Gross. They’re commenting on two reports on the FDA’s accelerated approval process, the path now for most new cancer drugs:
These articles serve as a reminder that the accelerated approval pathway is a permissive process that tolerates nonrandomized trial methods and a variety of outcome measures that bear an uncertain relationship to patient benefit. Even the nomenclature of these surrogate outcomes can be misleading to clinicians and patients. Response rate is not a measure of the rate of tumor regression but a measure of the proportion of patients who show a tumor response. This in turn is usually defined as more than 30% reduction using a scoring system that combines tumor measurements and markers at a particular point in time. Other commonly used surrogates include progression-free survival, time to tumor progression, disease-free survival, and recurrence-free survival. These terms overlap and once again can depend on which tests are performed at what time and how they are interpreted. The most important commonality across these measures is their lack of patient centeredness: the inability to reliably correlate these surrogates with outcomes that patients care about. Given the unsatisfactory nature of these surrogate outcome measures, it is of the greatest concern that the studies by Gyawali et al and Chen et al show that most of the drugs given accelerated approval have not been shown to improve overall survival in postmarketing trials.
It’s just mind-blowing to see so many cancer drugs approved with so little evidence of benefit. Emerson Chen and colleagues looked at 85 cancer drug indications approved on the basis of the surrogate endpoint of “response rate” — a measure of the percentage of cancer patients whose tumor shrinks beyond an arbitrary threshold.
Only 6 have since yielded evidence of an overall survival benefit. Many of the drugs have remained on the market for years without more definitive studies. In the trials that led to FDA approval, the median complete response rate was just 6%.
And guess what often happens when provisionally approved drugs fail to show survival or quality of life benefits? The FDA allows the status quo to continue for years, and it may even grant full approval:
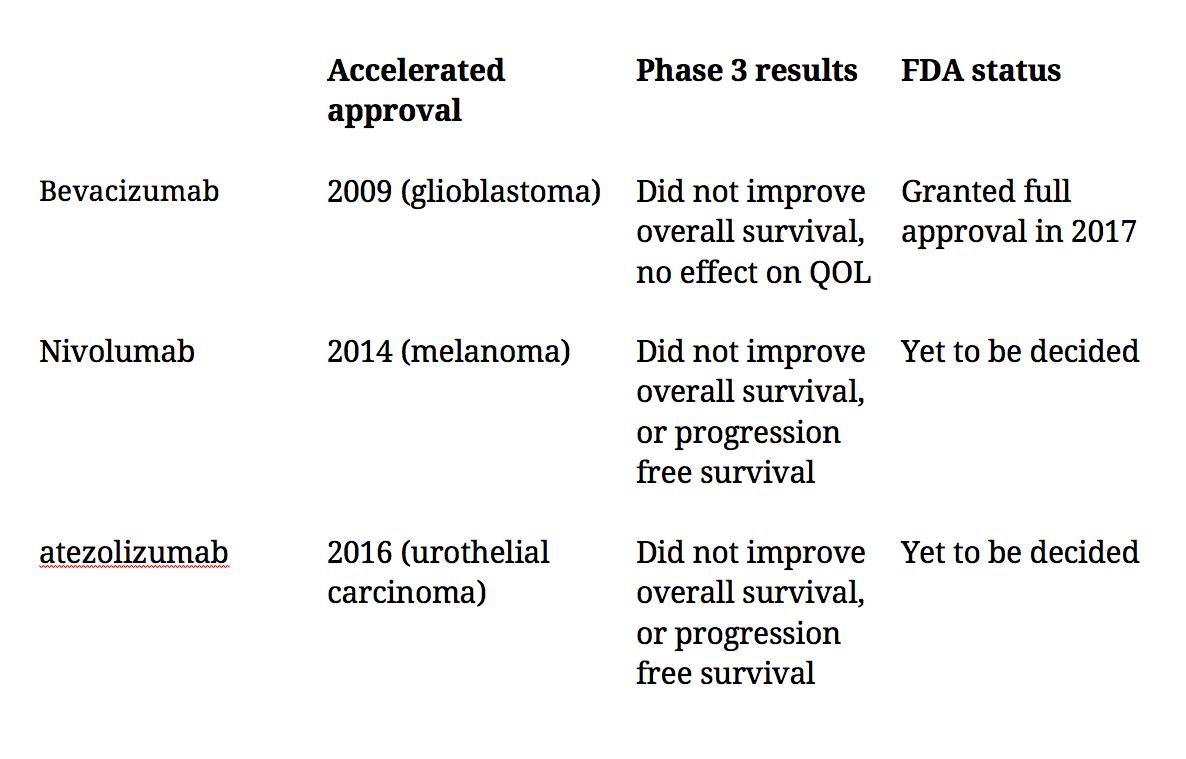
Bishal Gyawali and co-authors looked at 93 accelerated cancer drug approvals granted from Dec. 11, 1992, through May 31, 2017. In post-approval confirmatory trials, only 20% of the drugs have shown improvement in overall survival.
Why allow unrandomized trials that use surrogate endpoints? ASCO’s chief medical officer told NPR it’s “because these are rare cancers, or the drug targets a rare mutation” But the trials in Chen et al recruited a median of 117 subjects!
No doubt it’s hard to get patients to enroll in a well-designed confirmatory trial for a drug that’s already approved, as ASCO’s Richard Schilsky told NPR. But that to me seems like an argument to do better trials from the get go, not more unclear trials engineered to hasten FDA approvals.
